

Statins for Cholesterol — Friend or Foe?
As a Medication Management pharmacist, I often get questions about statin drugs for high cholesterol. Many people have heard negative things about statins, and are reluctant to take them. That's understandable - no one wants to take a medicine that causes more harm than benefit. But I've learned that many haven't explored BOTH the risks and benefits with their doctor or pharmacist. If you're faced with the decision about whether to use a statin, you'll want to know both sides of that story. In this post we'll talk in broad terms about risks and benefits of statins, and how to work with your doctor to decide what's right for you.
A little background
Statins are a group of drugs that lower blood cholesterol levels. They do it by inhibiting the body's ability to make cholesterol on its own. That's important because cardiovascular (CV) disease starts when cholesterol-containing plaques form inside arteries. When blood cholesterol is at safe levels, arterial plaque formation is less likely. But there's more. When plaques build up inside arteries, the body mounts an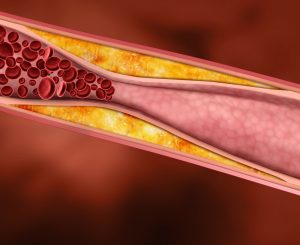 inflammatory response, and draws blood platelets to the area. The result can be a blocked (or partially blocked) artery. Statins not only decrease the chance of cholesterol-containing plaques forming, they also decrease the resulting inflammation and platelet overactivity. Overall, these and other effects result in a lower risk of heart attack, chest pain (angina) and stroke. At least one study showed that those who took a statin decreased their risk of heart attack and stroke by nearly 50%.
inflammatory response, and draws blood platelets to the area. The result can be a blocked (or partially blocked) artery. Statins not only decrease the chance of cholesterol-containing plaques forming, they also decrease the resulting inflammation and platelet overactivity. Overall, these and other effects result in a lower risk of heart attack, chest pain (angina) and stroke. At least one study showed that those who took a statin decreased their risk of heart attack and stroke by nearly 50%.
At the same time, CV disease is the leading cause of death in the United States and across the globe. In 2019, about 800,000 people died from heart disease and stroke in the US alone. Because CV disease affects so many people, the burden on the healthcare system and its related costs are huge. So from a population health viewpoint, the widespread us of statins makes a lot of sense. But what about individual health outcomes? We'll get to that in a minute.
There are several different statins, and they all work in the same way. The most common are atorvastatin, lovastatin, pravastatin, fluvastatin, rosuvastatin, and simvastatin. They' were prescribed to 35 million adults in the US in 2018. But surveys have shown that the majority of adults don't take them as prescribed, or simply refuse to take them at all. And that's largely because of worry over possible risks.
What are the potential risks of statins?
Every medication has side effects. Statins are no different. Here are the most common ones you may have heard about.
Muscle damage: This is the most concerning side effect for most patients I've talked with. Symptoms include muscle pain and weakness. Interestingly, studies in which patients didn't know if they were taking active drug or not showed a very low rate (5%) of muscle symptoms. But in non-research settings, nearly a third of those taking statins report muscle pain or weakness. Why is that? Well, there are a couple of possibilities. One is that real-world doses are simply higher than the doses used in research studies But many experts believe that a major reason is that patients have heard about muscle problems and expect it. The random muscle aches and pain that most middle-aged and older people get may be attributed to a new medication instead of exercise or over-exertion. One thing we do know, though, is that if a statin is the cause of muscle symptoms, they will resolve when the medication is stopped. More than that, most often they'll not recur if a statin is restarted. In most people, the occurrence of muscle symptoms while on a statin doesn't mean a statin can't still be used safely.
Memory loss: There's been some research that suggests statins might increase the risk of memory loss. So far the best research suggests that if memory loss happens after a statin is started, it will resolve when the statin is stopped. And memory loss might not recur if a statin is restarted. But the other interesting thing is that some research has shown that statins actually decrease the risk of dementia. So obviously there's a lot we don't know, and research continues.
Diabetes: Many people with risk factors for diabetes will ultimately develop diabetes over several years. It's pretty clear now that the risk of developing diabetes is slightly higher if those individuals are taking a statin. (Statins don't seem to cause that problem in people who aren't already at risk for diabetes.) But when those at risk for diabetes, heart attack and stroke were treated with a statin, they had far fewer heart attacks and strokes than those who weren't. So here's the thing -- the risk of developing diabetes might go up a little, but the risk of having a heart attack or stroke goes down a lot. Overall, in certain people, the risk of diabetes pales in comparison to the health benefits of statins..
But what about the benefits?
If you've been diagnosed with CV disease, you likely know you're at an increased risk of heart attack and stroke. Or maybe you don't have a diagnosis of CV disease, but you've been told you're at high risk because of other factors. It's important for you to know what your risk is, AND what puts you at risk.
If you've had a heart attack or a stroke, that automatically puts you in the highest risk category. It's estimated that 20% or more of those with heart attack or stroke will suffer another within five years. But if you haven't had an event, what may be putting you at risk? Well, doctors use a risk calculator that takes gender, age, cholesterol levels, blood pressure, smoking status, and diabetes into account. Together, these lifestyle and health factors provide an indicator of 10-year CV disease risk. So a 50-year-old man who has high cholesterol but doesn't smoke, have diabetes or high blood pressure has roughly 1 chance in 10 of having a heart attack or stroke over the next ten years. Take another 50-year-old man who has diabetes, high blood pressure and cholesterol, and smokes, and his risk is closer to 1 in 2 over the next ten years. Big difference. These two imaginary people would likely view the risk/benefit balance of statin treatment differently.
Shared decision-making
If you've read this blog before, you know that I'm a huge proponent of patients, doctors, and pharmacists working together to improve health outcomes. As part of that, talking about risks and benefits of medications is a top priority. When it comes to statin use, open discussions between you and your doctor can help you decide on where the risk/benefit balance falls for you as an individual.
First, talk with your doctor about what puts you at risk. Maybe you've already had a heart attack or a stroke. But maybe the factors that put you at risk are things you can (and are willing to) change. Increasing physical activity can improve blood pressure, cholesterol, and blood sugar. Losing weight for those who are overweight or obese, same thing. Smoking cessation all by itself can make a big difference in CV disease risk.
And then discuss how high your risk is. Are you in the highest risk group? Or is your risk much lower? Talk with your doctor about your risk tolerance, and listen to any concerns they have. Together, you can make a plan to ensure you get the best possible health outcomes. And be willing to revisit that plan regularly, as you age and as new research emerges.
Here's where your pharmacist can help
If you've decided to try a statin, your pharmacist can help. Share your goals and  concerns with your pharmacist. Later, if you suspect you're having side effects, have a talk with your pharmacist before you consider stopping it. There are a variety of ways to address side effects, and we can help find the best one for you. More than that, we'll be sure to keep your doctor in the loop.
concerns with your pharmacist. Later, if you suspect you're having side effects, have a talk with your pharmacist before you consider stopping it. There are a variety of ways to address side effects, and we can help find the best one for you. More than that, we'll be sure to keep your doctor in the loop.
And we can't leave out the subject of Pharmacogenetics. Pharmacogenetics looks at genetic differences in drug metabolism and elimination that may affect safety and efficacy. It's similar to ancestry testing, but looks at different types of genes. And it turns out that one gene-related difference can affect certain people ta king statins, making them more susceptible to side effects. If you're curious about your pharmacogenetic profile, BetterMyMeds can provide you with OneOme Pharmacogenetic testing and counseling. .Contact us for more information!
king statins, making them more susceptible to side effects. If you're curious about your pharmacogenetic profile, BetterMyMeds can provide you with OneOme Pharmacogenetic testing and counseling. .Contact us for more information!
As always, we invite you to add your comments and questions below. And you're always welcome to contact us directly at BetterMyMeds. We're committed to helping you get the best health outcomes from your meds!
![]()
Excellent article, Betty! Here are a couple of counseling points that I like to share:
1. Avoid eating grapefruit or drinking grapefruit juice when taking a statin, as grapefruit contains a component that can increase the risk of side effects.
2. If you feel you may be experiencing side effects from a statin, it does not mean that you necessarily would experience the side effects from another statin. The more commonly used statins are known as lipid-soluble. However, if experiencing side effects from one of these statins, it is possible to consider a water-soluble statin, which generally has a lower rate of muscle soreness associated with them.
Now a question for you, Betty. What are your feelings about taking a Co-Q10 supplement to potentially reduce side effects?
Which is better a statin or Repatha?
That is an excellent question, Deborah. Thank you for asking it!
Repatha belongs to a group of medications known as monoclonal antibodies, which are quickly becoming more-commonly used for treating numerous health conditions.
Repatha is generally reserved for patients with what is called familial (or hereditary) hypercholesterolemia, or for patients with established cardiovascular disease who did not respond to or tolerate statin therapy. Repatha is also very expensive, so many insurances will not cover Repatha until the provider has shown evidence that the patient has tried and did not respond well to at least two attempts with statin therapy.
Repatha also has some side effects. The most common ones include pain at the site of injection, some back pain, and flu-like symptoms.
So to answer your question, Deborah, I don’t necessarily consider Repatha to be better or worse than statins. However, statins do remain the therapy of choice to treat elevated cholesterol levels, with Repatha considered as an alternative for patients who do not respond well to or tolerate statin therapy.
Hey Alan! Thanks for your comments.
I agree that grapefruit juice has the potential to increase side effects from some of the statins, especially simvastatin. I do have many patients who really hate losing that particular fruit for the rest of their lives though, and have learned that research is kind of soft on just how much grapefruit or grapefruit juice is likely to cause a problem. I’ve often told patients who miss their grapefruit that as long as they partake in moderation, they’ll likely be ok. And the definition of “moderation” is likely different for every patient. A good thing for people to talk to their pharmacist about!
And hmmmm, Co-Q-10. As with so many dietary supplements, research hasn’t answered the question reliably. Theoretically, statins deplete the muscles of coenzyme Q10, so replacing it with a supplement should decrease muscle side effects. And some studies show that it does, but others show it doesn’t. Based on what I’ve seen I wouldn’t recommend it for prevention since most people never even get distressing muscle problems. For those who have muscle side effects, and have tried other statins or other dosing regimens without success, a trial of Co-Q-10 sure would make sense to see if muscle symptoms improve. What do you think? Maybe that’s a subject for a whole other post!
Betty
Your article about statins was of special interest to me. I take a 40 mg tablet of pravastatin every day. Some instructions are to take 1 tablet at bedtime. Is there a reason that it should be taken at bedtime vs. another time of day?
Thanks for this great question, Martha!
Our bodies manufacture more cholesterol during the night than the daytime. So it makes sense that doctors often tell patients to take their statin at night. But I don’t always hold fast to that rule when talking to patients, and here’s why:
First, it’s more important that a statin be TAKEN at all, which as I mentioned in the article doesn’t happen in a majority of people. So I often don’t get in the weeds about WHEN to take it.
Second, if a person has been on a statin for a while, and it’s doing its job, cholesterol numbers are at goal, then tweaking the time of administration isn’t likely to make a real difference.
Finally, it gets complicated. It matters more with statins that only stick around in the body for a short time, so lovastatin, pravastatin, simvastatin, and fluvastatin are more likely to respond to the nighttime dosing than the others.
What I usually tell patients is, if it fits in your schedule to take the statin at night and you can still adhere to the treatment plan, then by all means do that. If you’re more likely to take it consistently by taking it at another time of day, then take it at that time. And if your numbers are already at goal, it’s probably not an important issue for you.
Betty